Parkinson's Disease [PD]- its symptoms, diagnosis, and treatment (February 2025):
- Get link
- X
- Other Apps
Parkinson’s Disease (PD) - What is it? | |
| |
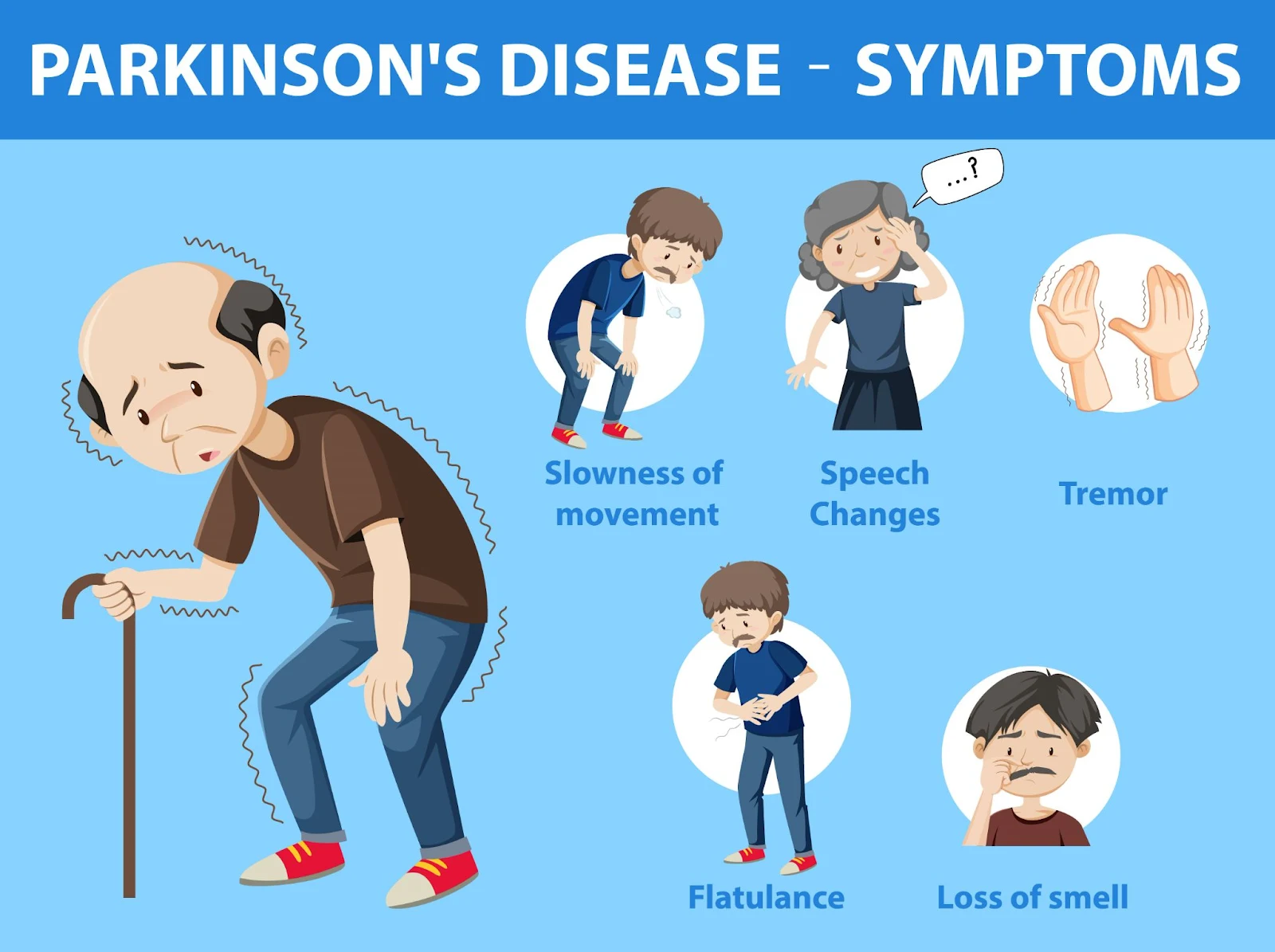
Symptoms of Parkinson’s Disease [PD]:
Both types of signs are listed below: Possible early non-motor (nonmovement-related) symptoms:
Major primary motor-related difficulties: (Motor impairment; movement-related) symptoms: Slowed movement (Bradikensia)-
Tremors (involuntary shaking of body parts) and rhythmic (back and forth motion) movement of muscles at rest :
Muscle rigidity, inflexibility, stiffness of the limbs, arms, legs, and trunk- or resistance to the movement -
Balance problem and tendency to fall - It is caused by abnormal movement of legs and/or arms, uncontrolled and unintended movements like shaking, stiffness, difficulty in balance, and mis-coordination of body parts. Secondary Symptoms: Some of the secondary symptoms of PD are listed below:
Other associated symptoms of Parkinson’s Disease [PD]: There may be several other associated symptoms of PD, some of which are listed below:
Note: Similar symptoms may be seen due to aging and/or some other reasons. Only a neurologist can diagnose, detect, and confirm Parkinson’s Diseases. | |
Know more about Parkinson’s dementia:
Symptoms of Parkinson’s disease dementia include:
Certain people are more likely to develop Parkinson’s disease dementia. Risk factors for the condition include:
| |
Causes of PD:
The exact cause of PD is still unknown, however, some of the possibilities are listed below:
Causes based classifications of Parkinson's disease [PD]: It can be classified as below: Familial Parkinson’s disease:
Idiopathic Parkinson’s disease: It is believed that the abnormal shape of a protein called alpha-synuclein is responsible for PD. When some proteins do not have the correct shape (called misfolding), such proteins cannot be broken and cannot be used by our bodies. Such unbroken and unused proteins build up. The tangles or clumps of such proteins are called Lewy bodies and cause toxic effects and cell damage. Induced Parkinsonism: Some diseases have similar symptoms to Parkinson's Disease [PD]. Such diseases are called Induced Parkinsonism ( not true Parkinson's Disease). The causes for such induced parkinsonism are listed below:
|
Diseases similar to PD: Many diseases/disorders show symptoms similar to PD. They are also called Parkinson's - plus syndrome or Atypical Parkinsonism because they have the symptoms of PD plus some additional symptoms. Some of them are listed below:
The big difference is that such disorders do not respond to Levodopa treatment like PD does. |
Which genes are linked to Parkinson’s Disease [PD]? Researchers have found that the following genes are linked with PD: SNCA
LRRK2:
DJ-1:
PRKN (Parkin):
PINK1:
GBA (Glucocererosidase-beta):
|
Diagnosis of Parkinson’s Disease (PD): A neurologist (a healthcare expert) can diagnose PD or rule out other conditions with the help of some examinations, procedures, and biological marker tests before the motor symptoms. It includes:
Now, we will describe the diagnosis: Physical and Neurological examination along with medical history:
Blood and lab tests:
Imaging tests:
SPECT scan ( DAT scan):
Genetic testing: Samples of blood, saliva, skin, tissue, or amniotic acid are taken to analyze changes in genes (DNA) and correlate with any family history of Parkinson’s disease and/or with your ongoing symptoms. Medications: Certain medicines for Parkinson’s disease are given to the patient. If medicine improves the condition, it helps to diagnose the disease correctly. Alpha-synuclein test:
SynONE test:
Follow-up appointments: Follow-up appointments with a neurologist are necessary to confirm the diagnosis, adjust the medications, and provide the most suitable treatment. | |
Stages of Parkinson’s Disease [PD]: It may be classified into four parts based on the Movement Disorder Society - Unified Parkinson’s Disease Rating Scale (MDS-UPDRS). It examines the symptoms and describes the impact of PD on different parts of the body. Part 1 (Nonmotor aspects of experiences of daily living):
Part 2 (Motor aspects of experiences of daily living)
Part 3 (Motor examination):
Part 4 (Motor complications):
|
Treatment of Parkinson’s Disease (PD): PD can not be cured, but by medications, its symptoms can be controlled.
Some of the medications are listed below: Dopamine:
Dopamine Simulators (Dopamine Agonists):
Dopamine Metabolism Blockers:
Levodopa metabolism inhibitors:
Adenosine blockers:
Medicines may also be given to impact other brain chemicals like neurotransmitters which transfer the information between the brain cells. Some medicines may be given to control the non-movement symptoms. Some of the medications available in the market are described below: |
Medicines: |
Carbidopa-levodopa [Rytary, Sinemet, etc.]:
Dosage:
Side effects:
|
Inhaled levodopa (Inbrija):
|
Dopamine agonists:
Some of the dopamine agonists are listed below:
Dosage:
Side effects of dopamine agonists:
Some more side effects include:
|
MAO-B inhibitors:
Some MAO-B inhibitors are listed below:
Dosage :
Side effects: Some of the side effects are listed below:
|
COMT inhibitors:
Some of the COMT inhibitors are listed below:
Dosage:
Side effects: Some of the side effects are listed below:
|
Anticholinergics:
Some of the Anticholinergics are listed below:
These medications are believed to be equally effective, but trihexyphenidyl and benztropine are the most commonly used. Dosage:
Side effects: Some of the side effects are listed below:
|
Amantadine (Symmetrel, and Gocovri):
Dosage:
Side effects: Some of the side effects are listed below:
|
Adenosine receptor antagonists (Adenosine 2A antagonists):
Dose:
Side effects :
|
Treatment by Surgery: When medications are no longer effective in controlling the symptoms of PD, the neurosurgeon may recommend surgery. The following types of surgery may be performed to treat the symptoms of PD: Stereotactic surgery in the thalamus, globus pallidus, and subthalamic nucleus part of the brain: Pallidotomy (lesion surgery) -
It is performed by inserting a wire probe into the globus pallidus – a very small region of the brain, measuring about a quarter inch, involved in the control of movement.
Thalamotomy:
Deep Brain Stimulation (DBS):
Side effects: Some of the side effects of DBS are listed below:
Pump-delivered therapy: Carbidopa-levodopa infusion (Duopa):
Side effects: Some risk is involved in placing the feeding tube. It may come out or cause an infection at the infusion site. |
Advanced treatment of Parkinson’s Disease [PD]: MRI-guided Focussed UltraSound (MRgFUS) is a minimally invasive treatment that is used to control the tremors related to Parkinson’s disease. In this procedure, an MRI is guided by ultrasound waves to the brain areas where the tremors start. The ultrasound waves with very high temperatures burn these areas. Side effects:
|
Treatment in the experimental stage: Some of the following treatments are in the experimental stage and may be available in the future: Stem cell transplant:
Neuron-repair treatments:
Gene therapies and gene-targeted treatments:
The following infusion formulations are also under trial:
Note:
|
Treatment for non-motor symptoms in PD: Always keep in mind that the particular medications and their dosages are always decided by the neurologist or health expert as per the needs of the individual. It varies from one person to another. However, a piece of general information is given here: Depression:
Sleep disorders:
Dementia
Psychosis and hallucinations
Pimavanserin (Nuplazid): It is used to treat the hallucinations and delusions that can occur due to Parkinson's disease. |
Lifestyle changes and home remedies to manage the symptoms of Parkinson’s Disease [PD]: We can not say that lifestyle and home remedies can cure PD. It is yet to be established whether caffeine, antioxidants, and other dietary factors may be beneficial for preventing or treating PD. However, with the help of lifestyle changes and home remedies, symptoms of PD may be managed to some extent.
Some of the lifestyle changes and home remedies are listed below: Healthy eating for PD patients: Parkinson’s Disease is the result of decreased dopamine levels in the brain.
These foods include:
Avoid dairy products and a high-intake protein-rich diet:
Physical activities and exercise:
|
Complementary and Supportive Therapies: Such therapies with medications help to manage the symptoms like fatigue, depression, and pain. They also improve the quality of life. Some of the such therapies are listed below: Massage: It can reduce muscle tension and provide relaxation. Tai chi:
Yoga:
Alexander technique:
Meditation:
Relaxation Technique:
Self-hypnosis:
Acupuncture:
Coping and support:
Some self-improvement techniques are also helpful:
Precautions for PD patients: Exercises: Very simple exercises and stretches may help you move around and walk more safely. However, some precautions needed to be taken, including:
Precautions to avoid falling:
Precautions while getting dressed:
The following tips help improve balance and gait:
The following tips help prevent falls:
|
What is the wearing-on and wearing-off condition of PD?
|
Is there a cure for Parkinson’s? There’s currently no cure for Parkinson’s disease. It is chronic and worsens over time. |
Parkinson’s prognosis: Complications from PD can greatly reduce the quality of life and prognosis. Individuals with PD can experience dangerous falls, as well as blood clots in the lungs and legs. These complications can be fatal. Proper treatment improves your prognosis and increases life expectancy. It may not be possible to slow the progression of Parkinson’s, but you can work to overcome the obstacles and complications to have a better quality of life for as long as possible. |
What is the life expectancy of PD patients: Parkinson’s disease is not fatal. However, in some cases, Parkinson ’s-related complications can shorten the lifespan of people diagnosed with the disease. The difference in the life expectancy of PD-affected people and people without PD may be negligible. |
Summary of the blog: |
General Summary:
|
Causes Summary:
|
Symptoms summary:
|
Diagnosis summary:
|
Treatment summary:
|
Treatment under trial to slow the progression of Parkinson’s Disease (PD):
|
|
|
General data summary:
|
USA data for PD:
|
Disclaimer: The best efforts are made to provide authentic and updated basic information on Parkinson's Disease. This blog is prepared from the data compiled from various websites including those mentioned in the blog. The information given in this blog is only for educational purposes, it is not intended to serve as medical advice and can not replace the medical advice in any form. Anyone seeking specific neurosurgical advice, medication, or assistance should consult a health care provider, neurosurgeon, or neurologist. Always keep in mind that the particular medications and their dosages are always decided by the neurologist or health expert as per the needs of the individual. It varies from one person to another. I am not a health professional, and this blog is not AI-generated, instead, it is manually written. Therefore I do not take any responsibility (legal or otherwise) for its typographical error, correctness, completeness, consequences, etc. Before following anything from this blog, it is strongly requested to consult a specialist, doctor, neurologist, or healthcare provider. https://my.clevelandclinic.org |
Parkinson’s disease is not curable and not fatal. It is possible to manage, control, and delay the progress and more severe symptoms of the disease. We may live life in a better way with the help of treatment. == Best of luck== ==The end== |
- Get link
- X
- Other Apps








Comments
Post a Comment
Thank you, most welcome, 👍